Cervical Spine Anatomy
The cervical spine consists of seven vertebrae (C1–C7) that form the neck and protect the spinal cord, which carries signals between the brain and the rest of the body.
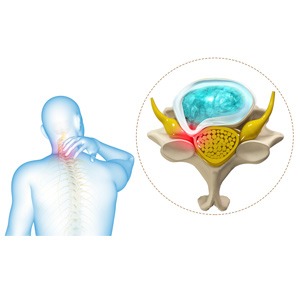
The spinal cord travels through the spinal canal, a protective bony tunnel within the vertebrae. When this canal becomes narrowed, the spinal cord may become compressed, which can interfere with normal nerve function.
Compression of the spinal cord in the neck is known as cervical myelopathy.
What Is Cervical Myelopathy?
Cervical myelopathy refers to dysfunction of the spinal cord caused by compression in the cervical spine. It is most commonly caused by degenerative changes in the spine, a condition often referred to as degenerative cervical myelopathy (DCM).
Over time, age-related changes such as disc degeneration, bone spurs, thickened ligaments, and spinal instability may narrow the spinal canal and place pressure on the spinal cord.
Unlike cervical radiculopathy, which affects individual nerve roots, cervical myelopathy affects the spinal cord itself, which can lead to more widespread neurological symptoms.
Incidence and Prevalence
Cervical myelopathy is the most common cause of spinal cord dysfunction in adults worldwide.
Research suggests:
- The estimated incidence is approximately 4–6 cases per 100,000 people per year.
- The prevalence may be at least 60 per 100,000 individuals, and likely higher due to underdiagnosis.
- The condition most commonly affects individuals over the age of 50.
Because symptoms often develop gradually and may initially be subtle, cervical myelopathy is sometimes diagnosed later in the course of the disease.
Causes of Cervical Myelopathy
The most common cause is degenerative narrowing of the spinal canal, but several structural changes may contribute.
Common causes include:
- Degenerative disc disease
- Cervical spinal stenosis
- Bone spurs (osteophytes)
- Thickening of spinal ligaments
- Cervical disc herniation
- Ossification of the posterior longitudinal ligament (OPLL)
- Congenital narrowing of the spinal canal
- Trauma or spinal instability
These conditions reduce the available space for the spinal cord and can lead to progressive compression.
Symptoms of Cervical Myelopathy
Symptoms often develop gradually and may worsen over time.
Common symptoms include:
- Difficulty with balance or walking
- Hand clumsiness or loss of fine motor skills
- Weakness in the arms or legs
- Numbness or tingling in the hands
- Neck pain or stiffness
- Difficulty with tasks such as buttoning clothing or writing
In more advanced cases, patients may develop:
- Frequent falls
- Coordination problems
- Muscle stiffness or spasticity
- Bowel or bladder dysfunction
Because the spinal cord controls many functions of the body, symptoms may affect both the upper and lower extremities.
Natural History and Progression
The natural history of cervical myelopathy varies among patients. Some individuals experience slow progression, while others may have periods of stability followed by worsening symptoms.
Studies suggest that:
- Many patients with untreated cervical myelopathy experience gradual neurological decline over time.
- Some patients experience stepwise worsening of symptoms.
- Neurological deficits may become permanent if spinal cord compression persists.
Because of the risk of progression, cervical myelopathy is often considered a condition that may ultimately require surgical treatment once symptoms develop.
Risk of Spinal Cord Injury
Patients with cervical spinal stenosis or cervical myelopathy have less space available for the spinal cord, which may make the spinal cord more vulnerable to injury.
Although serious spinal cord injury remains uncommon, research suggests that individuals with significant cervical stenosis may have a higher risk of neurological injury following trauma compared with people who have a normal cervical spinal canal.
Examples of trauma that could potentially cause injury include:
- Falls
- Motor vehicle accidents
- Sports-related impacts
For this reason, physicians may recommend avoiding high-risk activities or contact sports in patients with significant spinal cord compression.
Importantly, most individuals with cervical stenosis do not develop spinal cord injury, but the increased vulnerability of the spinal cord is one factor physicians consider when discussing treatment options.
Diagnosis
Diagnosis begins with a medical history and neurological examination.
Your physician may evaluate:
- Balance and walking ability
- Hand coordination and dexterity
- Muscle strength
- Reflexes and abnormal neurological signs
Imaging studies are used to confirm spinal cord compression.
Common diagnostic tests include:
- MRI scans, which show spinal cord compression and soft tissues
- CT scans, which provide detailed images of bone structures
- X-rays, which evaluate spinal alignment and instability
MRI is the most commonly used test to evaluate cervical myelopathy.
MRI Findings: Myelomalacia and Spinal Cord Signal Changes
Patients with cervical myelopathy sometimes see terms such as “increased signal within the spinal cord” or “myelomalacia” in their MRI reports.
These findings refer to changes within the spinal cord itself, which may occur when the cord has been compressed for a prolonged period.
On MRI, this may appear as:
- Increased signal intensity on T2-weighted images, indicating irritation or injury to the spinal cord
- In more advanced cases, myelomalacia, which refers to softening or structural changes within the spinal cord tissue
The presence of spinal cord signal changes can suggest more advanced or longstanding compression and may sometimes be associated with a greater risk of persistent neurological symptoms.
However, the significance of these findings varies among patients, and many individuals with signal changes still experience improvement after surgical decompression.
Your physician will interpret these MRI findings in combination with your symptoms and physical examination when discussing treatment options.
Treatment
Treatment depends on symptom severity and the degree of spinal cord compression.
Non-Surgical Treatment
In patients with mild symptoms, conservative management may include:
- Physical therapy
- Activity modification
- Anti-inflammatory medications
However, conservative treatment does not remove pressure from the spinal cord, and symptoms may progress over time.
Surgical Treatment
Surgery is often recommended when:
- Neurological symptoms are present
- Spinal cord compression is significant
- Symptoms are progressive
The goal of surgery is to decompress the spinal cord and prevent further neurological deterioration.
Common surgical procedures include:
- Anterior cervical discectomy and fusion (ACDF)
- Cervical disc replacement in selected patients
- Posterior cervical laminectomy and fusion
- Cervical laminoplasty
The choice of procedure depends on the location and extent of spinal cord compression.
Outcomes of Treatment
Several large studies have evaluated outcomes of surgery for cervical myelopathy.
One of the most influential research efforts is the AO Spine international studies on degenerative cervical myelopathy, led by Dr. Michael Fehlings and colleagues.
These landmark studies demonstrated that:
- Surgical decompression significantly improves neurological function and quality of life in many patients.
- Many patients experience improvement in walking ability, hand function, and overall mobility after surgery.
- Early surgical treatment is associated with better neurological recovery.
Long-term follow-up studies show that surgery generally halts disease progression and improves symptoms in the majority of appropriately selected patients.
Summary
Cervical myelopathy occurs when narrowing of the spinal canal compresses the spinal cord in the neck, leading to symptoms such as balance problems, hand clumsiness, weakness, and numbness. It is the most common cause of spinal cord dysfunction in adults and typically develops due to degenerative changes in the cervical spine. MRI studies may sometimes show signal changes within the spinal cord, which can indicate chronic compression. Early recognition is important because untreated spinal cord compression may lead to permanent neurological deficits. Surgical decompression has been shown in multiple landmark studies to improve neurological function, prevent further deterioration, and improve quality of life in many patients.