Thoracic Spine Anatomy
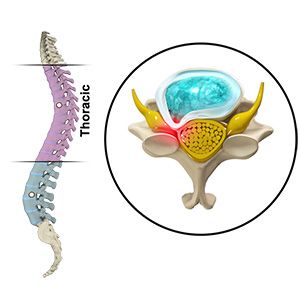
The thoracic spine is the middle portion of the spinal column and consists of twelve vertebrae (T1–T12) located between the cervical spine (neck) and lumbar spine (lower back). These vertebrae attach to the ribs and form the rib cage, which protects vital organs such as the heart and lungs.
The spinal cord travels through the spinal canal within the vertebrae and carries signals between the brain and the rest of the body. When the spinal canal becomes narrowed or a structure compresses the spinal cord in the thoracic spine, it can disrupt these signals and lead to neurological symptoms.
Compression of the spinal cord in this region is known as thoracic myelopathy.
What Is Thoracic Myelopathy?
Thoracic myelopathy occurs when the spinal cord becomes compressed in the thoracic spine. Because the spinal cord controls motor and sensory function below the level of compression, thoracic myelopathy can lead to symptoms affecting the lower extremities, balance, and walking ability.
Thoracic myelopathy is less common than cervical myelopathy, but when it occurs it can cause significant neurological symptoms because the thoracic spinal canal is relatively narrow and has less available space for the spinal cord.
Incidence and Prevalence
Thoracic myelopathy is relatively uncommon compared with spinal cord compression in the cervical spine.
Common causes such as thoracic disc herniation account for less than 1% of all disc herniations. Other conditions affecting the thoracic spine, including ligament ossification and spinal tumors, may also lead to thoracic spinal cord compression.
Because symptoms may develop gradually and mimic other neurological or orthopedic conditions, thoracic myelopathy may sometimes be diagnosed later in the course of the disease.
Causes of Thoracic Myelopathy
Several conditions may compress the spinal cord in the thoracic spine.
Common causes include:
- Thoracic disc herniation
- Degenerative disc disease
- Thoracic spinal stenosis
- Ossification of the ligamentum flavum
- Ossification of the posterior longitudinal ligament (OPLL)
- Spinal tumors or cysts
- Trauma or spinal fractures
- Congenital narrowing of the spinal canal
Thoracic disc herniations most commonly occur in the lower thoracic spine (T8–T12).
Symptoms of Thoracic Myelopathy
Symptoms often develop gradually and may worsen over time as spinal cord compression progresses.
Common symptoms include:
- Difficulty with walking or balance
- Weakness in the legs
- Numbness or tingling in the legs
- Sensory changes below the level of compression
- Muscle stiffness or spasticity
- Back pain in the mid-back region
In more advanced cases, patients may develop:
- Progressive difficulty walking
- Loss of coordination
- Bowel or bladder dysfunction
Because the thoracic spinal cord controls nerves to the lower body, symptoms often involve the legs and gait rather than the arms.
Natural History and Progression
Thoracic myelopathy is typically a progressive condition. As spinal cord compression persists, neurological symptoms may gradually worsen.
Patients may experience:
- Gradual decline in walking ability
- Increasing weakness or stiffness in the legs
- Progressive balance difficulties
Without treatment, ongoing spinal cord compression may lead to permanent neurological deficits.
Early diagnosis and treatment are important to help prevent further neurological deterioration.
Diagnosis
Diagnosis begins with a medical history and neurological examination.
Your physician may evaluate:
- Walking pattern and balance
- Muscle strength in the legs
- Sensation and reflexes
- Signs of spinal cord dysfunction
Imaging studies are used to confirm spinal cord compression.
Common diagnostic tests include:
- MRI scans, which show the spinal cord and soft tissues
- CT scans, which provide detailed images of bone structures
- X-rays, which evaluate spinal alignment and degenerative changes
MRI is the most commonly used test to evaluate thoracic spinal cord compression.
Treatment
Treatment depends on the severity of symptoms and the underlying cause of spinal cord compression.
Non-Surgical Treatment
In patients with mild symptoms, conservative management may include:
- Activity modification
- Physical therapy
- Pain management medications
However, conservative treatment does not remove compression from the spinal cord, and symptoms may continue to progress.
Surgical Treatment
Surgery is often recommended when:
- Significant spinal cord compression is present
- Neurological symptoms are progressive
- Walking ability or balance is affected
The goal of surgery is to decompress the spinal cord and prevent further neurological decline.
Surgical treatment may involve removal of the compressive structure, such as a herniated disc, thickened ligament, or bone spur.
In some cases, particularly when large portions of bone are removed or spinal instability is present, the procedure may also require spinal fusion to stabilize the spine.
Summary
Thoracic myelopathy occurs when the spinal cord becomes compressed in the thoracic spine, leading to neurological symptoms such as difficulty walking, weakness in the legs, and balance problems. Although less common than cervical spinal cord compression, thoracic myelopathy can cause progressive neurological decline if untreated. Imaging studies such as MRI are used to diagnose the condition and identify the cause of compression. While mild symptoms may sometimes be managed conservatively, surgical decompression—with or without spinal fusion—is often recommended to relieve pressure on the spinal cord and prevent further neurological deterioration.